Pearls of Knowledge: Third degree AV Block

Dysrhythmias: Third-degree AV Block
Pearls of Knowledge © BrainyNurses.com
Third-degree AV block is a complete failure of electrical conduction. No sinus or atrial impulses reach the ventricles, and complete AV dissociation occurs. Results in a slow ventricular rate with activation from a backup pacemaker. The ventricles may be activated by an impulse close to the AV node (narrow complex QRS) or from the purkinje fibers (wide complex QRS).

When third-degree block develops gradually, the patient may be symptomatic, but stable. If it occurs suddenly, the patient will most likely be unstable. The course is unpredictable, and treatment must be quickly implemented, especially in the setting of an acute MI. Treatment is a pacemaker.
Rhythm analysis
The SA node will fire regular P waves, but they are completely dissociated, and none are “married” to the QRS complexes. The QRS will occur at regular intervals and the rate and width of the QRS complexes will be...
Pearls of Knowledge: Breath sounds

Assessment: Breath Sounds
Pearls of Knowledge © BrainyNurses.com
The evaluation of breath sounds is part of most assessments. As you listen to breath sounds, remember the importance of listening to the front and back of the chest. Anterior assessment allows you to hear the upper lobes and right midlobe. Posterior assessment primarily allows you to hear the lower lobes.

Chest auscultation
With assessment, it is important to listen through inhalation and exhalation. The sequence should be side to side and top to bottom. For the elderly, it is recommended to listen to the lower lobes first to maximally hear abnormalities as they may tire with multiple forced breaths. To maximally expand the chest, have the patient lean forward to listen to the posterior chest and lean back to listen to the anterior and lateral chest.
Crackles
Crackles are heard on inspiration and indicate fluid, atelectasis,...
Pearls of Knowledge: Reentry

Interpreting Rhythms: Reentry
Pearls of Knowledge © BrainyNurses.com
Reentry is one of the most common causes of supraventricular and ventricular rhythms. It is seen with atrial fibrillation, atrial flutter, and runs of beats such as in ventricular tachycardia or paroxysmal atrial tachycardia.
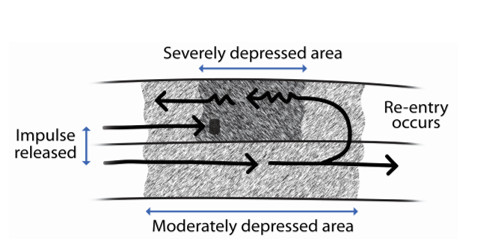
Typically, the myocardial tissue is depolarized and then becomes refractory. In patients with structural heart disease, or scar tissue from ischemia or infarction, a change in conduction occurs in some of the myocardial tissue and the tissue is not depolarized at the same time. Reentry occurs when a portion of the tissue is reactivated by an impulse that had already stimulated it.
Local reentry
Local reentry occurs within a small area (single site) of the atrium or ventricle such as atrial flutter, ventricular tachycardia, or paroxysmal atrial tachycardia. In atrial...
Pearls of Knowledge: AV Dissociation

Dysrhythmias: AV Dissociation
Pearls of Knowledge © BrainyNurses.com
AV dissociation occurs when there are two pacemakers present in the heart, usually for a relatively short period of time. The rate of the atria and ventricles will be very similar, but they are not “married”. The rhythm is easy to mistake for third-degree heart block.

Generally, the P waves will appear to “fade” into the QRS complexes and come out the back.

Rhythm analysis
(The P waves fade into the QRS and come out the back. The P waves are caused by the SA node. The QRS complexes are coming from the AV junction since the QRS is a normal duration.)

Pearls of Knowledge: Detecting Murmurs

Advanced Heart Sounds: Detecting Murmurs
Pearls of Knowledge © BrainyNurses.com
To elevate clinical practice, health care professionals should be listening to all four areas of the heart valves during an assessment.
In acute conditions, listening to heart sound is very important on presentation and then with subsequent assessments. If heart sounds change, it generally signifies a deterioration in condition such as ischemia or infarction (especially with inferior wall), or rupture of a papillary muscle, or the perforation of the intraventricular septum due to scar tissue.
Four areas of the valves to listen to:
- Aortic: 2nd ICS, right sternal border
- Pulmonic: 2nd ICS, left sternal border
- Tricuspid: 4th ICS, left sternal border
- Mitral: 5th ICS, left midclavicular line under the breast

Murmurs may be innocent or benign, all of which will be systolic murmurs.
- Innocent murmurs are heard in children, adolescents,...
Pearls of Knowledge: Anemia and Hydration

Lab Values: Anemia and Hydration
Pearls of Knowledge © BrainyNurses.com
The CBC with differential is a frequently ordered lab test and provides much information regarding infection, anemia, coagulation, and hydration. When bone marrow suppression occurs, low levels of red blood cells, white blood cells, and platelets will be seen.

Monitoring anemia
Anemia is seen frequently in many different types of patients. When the red blood cells are low, pallor will be seen. If the red blood cells are too numerous, such as in polycythemia vera, the blood is “thicker” and there is a risk for blood clotting and myocardial dysfunction due to the strain.
Men have a higher red blood cell count mostly due to hormonal differences which stimulate higher hemoglobin production and greater muscle mass. For ease in clinical practice, it is helpful to remember the normal level for hemoglobin for everyone is...
Pearls of Knowledge: Junctional Rhythms

Dysrhythmias: Junctional rhythms
Pearls of Knowledge © BrainyNurses.com
In junctional rhythm, the SA node is no longer in control and the AV node becomes the pacemaker by default due to the property of automaticity. Because the AV node is a less reliable pacemaker, the development of junctional rhythm is cause for concern. The analysis of junctional rhythms is determined by the P waves and the rate.

Because the impulse starts in the AV node, the atria are depolarized in a retrograde manner resulting in an inverted P wave in the upright (positive) leads (such as lead II).

Analysis of inverted P waves (in the upright leads)
- Inverted P wave before the QRS when the atria depolarize before the ventricles.
- Inverted P wave buried in the QRS when the atria and ventricles depolarize at the same time.
- Inverted P wave after the QRS when the ventricles depolarize before the...
Pearls of Knowledge: Second-degree AV Blocks

Dysrhythmias: Second-degree AV Blocks
Pearls of Knowledge © BrainyNurses.com
A defect in the AV node causes sinus rhythm with second-degree AV block, type I. Transmission takes longer with each successive impulse until one fails to be conducted to the ventricles. The PR interval gets progressively longer until some sinus impulses are blocked by the AV node. The rhythm usually occurs in a cyclic pattern such as 3:2, 5:4, etc. It is usually a temporary disorder and does not necessitate a pacemaker because it is not progressive.

A defect below the AV node in the Bundle of His or bundle branch system due to ischemia or injury causes second- degree AV block, type II. The sinus impulses are usually blocked at regular intervals, allowing only every second, third, or fourth impulse to be conducted to the ventricles. The PR intervals which are present will be constant. 2:1 conduction is common in second-degree,...
Pearls of Knowledge: Friction Rubs

Assessment: Friction Rubs
Pearls of Knowledge © BrainyNurses.com
Friction rubs are dry, cracking, and grating sounds caused by inflamed, roughened surfaces rubbing together. Due to the irritation in pericarditis and pleurisy, effusions will develop, and the friction rub will no longer be heard. The friction rub, heard early in the course, may be transient in both conditions and can cause significant pain.

Pericardial friction rub
- Heard during S1 and S2.
- Heard during inhalation and exhalation.
- Loudest at the apex and left sternal border.
- Heard best in the left lateral position or when leaning forward.
- Will be present in pericarditis and cardiac contusion.
Pleural friction rub
- Heard only on inhalation.
- Will be present in pleurisy and pulmonary embolus with pulmonary infarction.
Summary
So, the next time you hear a “grating” sound in the chest during your assessment, have the patient...
Pearls of Knowledge: SA Nodal Dysfunction

Advanced Dysrhythmias: SA Nodal Dysfunction
Pearls of Knowledge © BrainyNurses.com
The SA node is composed of P cells. Blood supply is from the SA nodal artery which is easily damaged. When damaged, ischemia results, fibrosis develops, and the node becomes dysfunctional. Initially the dysfunction may produce only mild symptoms, depending on the rate and duration of pauses. In more advanced disease, dizziness and possible syncopal episodes may be seen.
Three types of SA nodal dysfunction are covered here. They include abnormal overdrive suppression, sinus arrest, and sick sinus rhythm. With sick sinus syndrome the problem may be in the SA node or in the AV node.

Overdrive Suppression
In normal conduction, when an early beat occurs (such as a PAC), there is a pause in the rhythm. In healthy hearts, the conduction system “resets” itself and the rhythm resumes after the early beat....